| |
|
||
| Home | About | Contact | Vitamins for Schizophrenia |
|
|
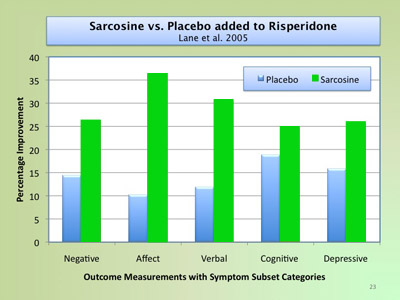
Sarcosine Therapy - A New Complementary Direction for Schizophrenia Treatment? | ||||||||||
|
Summary by Erin Hawkes, MSc
Sarcosine (N-methylglycine) is an amino acid made in the body from choline (a type of B vitamin). Sarcosine occurs naturally in the body when choline is changed to glycine (another amino acid). Sarcosine prevents glycine from being taken back into the brain cells from which it was released. This action changes the activity of its receptors by keeping more of the helper molecule glycine ready to help stimulate other brain cells via their NMDA (N-methyl-D-aspartate) receptors that can, among other roles, modulate memory. In quite a number of clinical trials sarcosine has been shown to be helpful in mitigating some of the negative symptoms of schizophrenia , something few other compounds or drugs have been shown to do.
The image above is a summary of the results from the Sarcosine clinical by Lane, et al, 2005. Effective Dosage: 2 grams daily. (Start with 1 gram per day, and slowly increase to 2 grams per day over a period of 2 weeks). 1 Gram may work in some people and may be the optimal dose for those people. Some people seem to prefer the effects of taking 50% of the daily dose in the morning at breakfast and 50% in the afternoon.Personal Experiences: You can see the ongoing discussion of people's experiences with Sarcosine in our discussion forums at this link: Forums: Sarcosine use for Negative Symptoms. Research: High-quality, reputable meta-analysis and randomized double-blind, placebo-controlled studies. Risks: Side effects are uncommon, relatively mild (e.g., sedation), and often resolve on their own. Note: A recent (2014) case study reported that a person received excessive stimulation from 2 grams per day, and so backed off to 1 gram per day and at that level found the benefits to be significant without excessive aggitation. It seems that some people may benefit from only 1 gram per day of Sarcosine. Selected references: 1. Singh SP, and Singh V. Two Grams of Sarcosine a day, is it too much? CNS Drugs. 2011;25:859-885. This is a report on one situation with sarcosine treatment for schizophrenia. After obtaining an informed consent, the doctors started administration of 2 g of sarcosine per day to treat persistent negative and cognitive symptoms. The patient's activity and mood improved within 2 weeks, but in the following 2 weeks the patient reported increased drive, activity, libido, unpleasant inner tension, and irritability. The doctors ruled out hypomania and decided to decrease the daily dose of sarcosine to 1 g, which resulted in reduction of drive and irritability. 2. Singh SP, and Singh V. Meta-analysis of the efficacy of adjunctive NMDA receptor modulators in chronic schizophrenia. CNS Drugs. 2011;25:859-885. A meta-analysis is a study that examines multiple individual studies using statistics. Singh and Singhs work included 1253 cases from 29 studies that were randomized, double-blind (neither psychiatrist nor patient knew which treatment the patient received), and placebo-controlled, making their results solid. They found sarcosine to be moderately effective in reducing a variety of symptoms of schizophrenia, such as those measured by the PANSS-N (Positive and Negative Syndrome Scale Negative symptoms; e.g., flat affect, apathy, and social withdraw). In conclusion, there is growing evidence for substances such as sarcosine to be therapeutic add-on therapies (except for clozapine). 3. Lane HY, Lin CH, Huang YJ, Liao CH, Chang YC, and Tsai GE. A randomized, double-blind, placebo-controlled comparison study of sarcosine (N-methylglycine) and D-serine add-on treatment for schizophrenia. Int J Neuropsychopharmacol. 2010;13: 451-460. Sarcosine or placebo was given to 60 patients in a double-blind, placebo-controlled study. All measures of outcome were positive for those receiving sarcosine, including Quality of Life and Global Assessment of Functioning as well as other standard tests of symptoms of schizophrenia. Sarcosines function is to keep certain messenger molecules (neurotransmitters) near their receptors for longer stimulation than the helper molecule D-serine does for these same receptors. The authors concluded that the treatment of schizophrenia with sarcosine would, in at least some cases, enhance patient functioning. 4. Lane HY, Liu YC, Huang CL, et al. Sarcosine (N-methylglycine) treatment for acute schizophrenia: A randomized, double-blind study. Biol Psychiatry. 2008;63: 9-12. This was a double-blind study of 20 people who had schizophrenia and were drug-free. During the 6-week experiment, patients received either 2 grams or 1 gram of sarcosine per day. The 2g/day group showed lessening of symptoms, suggesting that sarcosine is therapeutic at this dose (but not the 1g/day). Minor side effects (e.g., sedation, weight gain) were mild and brief. Sarcosine In-Depth Report
As science reveals more and more about the underlying pathophysiology
of schizophrenia, clinicians are advancing past simply treating visible
symptoms to attempting to correct the abnormalities themselves. The progression
of anti-psychotic medications clearly reveals this trend - while a sedative
dose of chlorpromazine was the treatment of choice fifty years ago for
psychotic diseases, emerging medications within the last decade target
specific neurotransmitter receptors in the brain with varying degrees
of specificity. The action of these newer medications allows for more
specific treatment of symptoms, with fewer of the side effects caused
by general-action systemic drugs. Emerging theories of what might cause schizophrenia (the "etiology"
of schizophrenia) also necessarily dictate what pharmacological treatments
might be most effective. In the 1950s and 60s, the dopamine hypothesis
was the leading "schizophrenia cause" theory, and treatments
of choice (for example, chlorpromazine) were generalized dopamine (D2)
receptor antagonists. This theory has since been expanded and modified,
leading to the development of atypical antipsychotic drugs that target
the different classes of dopamine receptors to differential degrees. However, a new emerging theory on the cause of schizophrenia is moving
away from pure dopamine, and shifting focus towards NMDA-type receptors
that use glutamate as a messenger. Greater understanding of NMDA function
and dysfunction is raising the possibility that sarcosine and glycine, essential
cofactor molecules for NMDA receptors, may improve the function of these
receptors in the brains of schizophrenia patients. Some researchers are
postulating that targeting NMDA receptors may alleviate positive, negative,
and cognitive symptoms of schizophrenia. Although the science is still
in its early stages, clinical trials of sarcosine and glycine treatment for schizophrenia
patients have both provided evidence for the NMDA dysfunction theory,
and have also indicated that these receptors are worth investigating as
key therapeutic targets. The Dopamine Hypothesis - Beginning to Understand
Schizophrenia as a Brain Disorder Although it is true - especially in our current stage of understanding
- that developing theories of etiology drive the development of newer,
more specific drugs, sometimes the order is reversed. This is certainly
what occurred in the 1950s, when the French physician Laborit synthesized
chlorpromazine as a general autonomic stabilizer. To the surprise of everyone,
chlorpromazine greatly improved the functioning of psychotic patients,
so much that they were often able to return to the care of their families. The success of chlorpromazine, and an understanding of its mechanism
of action in the brain, is what led to the first comprehensive theory
of schizophrenia causality (etiology).
Scientific testing of the compound revealed that it acts by blocking dopamine
receptor sites in the brain, preventing dopamine from binding and sending
chemical messages down brain circuits.
The image above is a model of dopamine neuron synapses in the brain. Dopamine neurons can be thought of like circuits that send electrical "messages" down long processes called axons; these messages produce different behaviors, depending on where they are directed. Synapses are like physical breaks in the circuit, where the electrical message is converted to chemical messengers (called neurotransmitters) and carried across the space to the next neuron in the circuit. Neurotransmitters are essential for sending these brain messages, and blocking neurotransmitters from interacting with the next neuron is one way to reduce activity in a particular circuit. Shown above is how an antipsychotic (neuroleptic) drug
such as chlorpromazine might physically block dopamine (the black circles)
from interacting with the next neuron. A is before the administration
of the drug (the white circles). B is after the drug has been administered.
(Image taken from the following website) The realization of the action of chlorpromazine, along with other early
neuroleptics, crystallized into the Dopamine Hypothesis of schizophrenia.
If dopamine receptor blockers helped alleviate some of the symptoms, then
perhaps schizophrenia was caused by too much activity in the brain’s
dopamine circuits. Scientists also noted that drugs such as amphetamines
and LSD produced hallucinations in healthy subjects, and worsened the
psychotic symptoms of people with schizophrenia. Because these drugs are
dopamine agonists
- meaning that they enhance dopamine activity - the fact that they induced
hallucinations seemed to be evidence for the Dopamine
Hypothesis. However, further scientific observations have revealed that the Dopamine
Hypothesis is not a complete etiological explanation for schizophrenia.
Increased dopamine is associated with positive symptoms but not all people
with schizophrenia experience the psychotic symptoms. For those whose
symptoms appear gradually, or who tend towards the negative or cognitive
end of the symptom spectrum, traditional neuroleptics that primarily target
dopamine receptors do not alleviate all of the symptoms. More recent research has suggested that other neurotransmitters and other
brain areas are implicated in schizophrenia (Maguire 2002). Serotonin,
GABA, and glutamate dysfunction may help explain some of the negative
and cognitive symptoms. Many of the newer atypical antipsychotics mediate
serotonin action, along with dopamine. Their effects depend on their ability
to decrease neurotransmitter activity in only certain parts of the brain,
while increasing it in others. NMDA Hypothesis - A unifying proposal? There are strong lines of evidence indicating that dysfunction of NMDA
receptors may explain the pathophysiology of positive, negative, and cognitive
symptoms of schizophrenia [Javitt and Coyle, 2003]. NMDA receptors are
located all over the brain, and are critical to learning, memory, brain
development, and general neural processing. Thus, NMDA receptor malfunction
could be a key in what some researchers are calling a "disorder of
the synapse" [Harrison and Weinberger, 2005]. Among other things,
the receptor modulates dopamine release from other neuron circuits; thus,
the NMDA hypothesis extends rather than negates previous findings concerning
dopamine. Normal NMDA receptor activity depends on three key factors: the binding
of glutamate to the receptor site, a depolarization (increase in positive
charge that indicates neuronal activation) of the neuron membrane in which
the receptor is embedded, and the presence of glycine. Glycine is an essential
cofactor for NMDA receptors; without it, the receptor does not work properly.
It is sarcosine and glycine that is the focus of many proposed therapies to enhance
NMDA activity in the brains of people with schizophrenia. The first evidence of a role for NMDA receptors in schizophrenia appeared
in a manner very much like that for the dopamine hypothesis; through the
observation of subjects given a chemical compound that altered normal
NMDA signaling. When healthy volunteers were given a dose of ketamine
(a drug that blocks NMDA receptor activity), they showed a wide variety
of commonly seen schizophrenia symptoms (Begany 2004, Javitt and Coyle
2003). Besides replicating the psychotic positive symptoms, subjects showed
a spectrum of negative symptoms, neurocognitive impairment, impaired eye-tracking,
and neuronal potential abnormalities (these last two signs have been observed
in schizophrenia patients during various studies). Further studies have
shown that people with schizophrenia may have increased levels of a natural
NMDA receptor antagonist (a chemical abbreviated as NAAG) in their prefrontal
cortex, temporal cortex, and hippocampus (Begany 2004, Coyle and Tsai
2004). More studies have indicated that low levels of glycine could be a key reason why NMDA activity is impaired in people with schizophrenia. Hashimoto et al (2003) reported reduced plasma levels of d-serine (another molecule naturally occurring in the body that can occupy the glycine binding site on the NMDA receptor and exert the same effects) in subjects with schizophrenia. Several genes that have been linked to increased risk for schizophrenia encode for enzymes that regulate the levels of d-serine in the body (Begany 2004). Increased expression of these genes might cause excessive degradation of d-serine in people with schizophrenia, resulting in decreased NMDA receptor activity. These and other genes implicated in schizophrenia heritability have also
been linked to the complex regulation of normal glutamate signaling activity;
this appears to occur through various mechanisms, including the role of
NMDA receptors (Harrison and Weinberger, 2005). The genetic evidence is
extremely hard to interpret, as the genes studied tend to produce proteins
that perform multiple roles throughout a person's lifespan. However, among
those roles is a regulation of glutamate signaling. Indeed, Harrison and
Weinberger [2005] propose that "genes predispose, in various ways
but in a convergent fashion, to the central pathophysiological process:
an alteration in synaptic plasticity, especially affecting NMDA receptor-mediated
glutamatergic transmission..." Implications for Treatment - Sarcosine and Glycine May Indirectly
Improve NMDA function Some exploratory research has examined possible ways to improve NMDA
receptor dysfunction. The goal, according to Dr. Joseph Coyle of Harvard
Medical School, "should be to stimulate the receptor indirectly at
the glycine modulatory site. You would not want to directly activate it
because if you overactivate it you will kill neurons" [Begany 2004].
Interestingly, the effects of NMDA-receptor antagonists in animal models
have shown a significant increase in glutamate release, possibly because
the body is attempting to compensate for reduced signaling by releasing
more of the messenger [Moghaddam and Jackson, 2003]. Excessive levels
of glutamate may then overload other (non-NMDA) glutamate receptors, causing
excitotoxicity and cell death. This is an interesting mechanistic proposal
for how NMDA receptor dysfunction may lead to poor synapse connections
and brain tissue atrophy in schizophrenia patients. One possible way to indirectly improve NMDA receptor function is to increase the availability of the receptor co-factor glycine. Studies using sarcosine and glycine or glycine-like molecules (such as d-serine and d-cycloserine) have shown very promising results. A series of double-blind, placebo-controlled crossover studies by Javitt and colleagues (as reported in Coyle 2004) administered 30-60 g/day of glycine to schizophrenia patients on traditional neuroleptic. Each group of patients received either placebo or glycine for 4 weeks; for the following 4 weeks, the original placebo group was given glycine as well. Results reported a significant decrease (17%) in negative and cognitive
symptoms for the glycine group, and for the placebo group following the
4-week crossover. In another crossover study by Javitt et al, the group
that received glycine first (for six weeks) and then switched over to
placebo (taken for another 6 weeks after a two-week washout period) maintained
the improvements achieved during glycine treatment, suggesting that the
therapeutic effects may be relatively enduring. These results were replicated
by Heresco-Levy et al (1999) using a similar cohort of schizophrenia patients
taking neuroleptic medications; results from the groups receiving glycine
showed a gradual but significant reduction in negative and cognitive symptoms
(up to 30%), but no effect on positive symptoms. Again, those who switched
over placebo maintained the original benefits of glycine treatment throughout
the placebo period. Other studies have looked at the effects of d-serine and d-cycloserine.
Interestingly, d-serine appeared to improve positive symptoms as well
as negative and cognitive in schizophrenia patients who did not respond
well to traditional neuroleptics (study by Tsai et al 1998, quoted in
Coyle et al 2004). D-cycloserine, when added to first-generation antipsychotic
treatment, showed maximum benefits (measured by reduction in negative
symptoms) at a 50mg/day dose (the study tested 5mg-250mg/day - see Coyle
2004 for details). Other studies have replicated these findings (see Coyle
2004). Metabolic tests on the subjects of these studies revealed significantly
increased serum levels of sarcosine, glycine (or d-serine, depending upon the treatment
administered), the rise of which corresponded to the reduction of negative
symptoms. Coyle [2004] notes that "those with the lowest serum glycine
levels at baseline exhibited the greatest improvement with glycine, a
finding independently reported in studies with the partial agonist, d-cycloserine."
This indicates that supplemental sarcosine (N-Methyl Glycine) and glycine treatment may not help everyone;
a baseline test of glycine/d-serine levels before changing the treatment
regimen could help determine who would benefit the most. Special Consideration - Sarcosine and Glycine Interaction
with Clozapine Oddly enough, some of the same studies above reported a worsening of
negative symptoms in patients treated with d-cycloserine who were already
taking clozapine. D-cycloserine is the only partial glycine-modulatory
site agonist - d-serine and glycine are both full agonists. Partial agonists
can also be thought of as partial antagonists, because they occupy the
modulatory binding site and prevent full agonists, that might maximize
NMDA receptor function, from binding. Therefore, the NMDA receptor with
a bound partial agonist is limited to only the level of activity that
the partial agonist can facilitiate, which is better than average, but
not the maximum. Interestingly, the full agonists did not show any effects
(beneficial or detrimental) in subjects taking clozapine. Coyle [2004]
suggests that because clozapine already alters the glycine modulatory
site on NMDA receptors to allow full occupancy, the presence of additional
agonists such as glycine and d-serine do not provide any additional benefit
(because the modulatory sites are alreadly occupied). Moreover, a partial
agonist like d-cycloserine, in the presence of already fully-occupied
glycine-modulatory sites (due to clozapine action), would only serve to
displace some of these occupied sites, because of this partial agonist/antagonist
property, thus explaining the worsening of negative symptoms. Conclusion - A Future for Sarcsosine and Glycine? The data seems to indicate that, at least for some people, sarcosine, glycine or
d-cycloserine treatment added to a standard regimen of antipsychotics
could have substantial benefits in terms of mitigation of schizophrenia’s
negative symptoms. Early studies have indicated as much as a 24% to 40%
improvement in negative symptoms with glycine. (However, D-serine has
been reported to cause renal tubular necrosis in rodents; thus, it is
still under toxicology investigation by the FDA.) We are not aware of the current clinical trials studying these compounds
(companies may be doing studies that they have not publicized). In summary, the potential benefits from sarcosine and glycine seem significant and the risks associated with them seems low (based on trials conducted to date, and detailed glycine information we've reviewed). However the research into sarcosine and glycine's value in treating schizophrenia is still relatively early in the testing phase. If you are interested in trying sarcpsome pr glycine, we highly recommend you print out this page and give it to your psychiatrist for his or her review and expert opinion on the best course of action given your situation and medical needs. Dr. Dan Javitt, one of the leading researchers/developers
of glycine supplementary treatments for schizophrenia (and who is cited
many times in this paper), was kind enough to answer some interview questions
for us about his work with glycine and the evidence for glycine treatments
for schizophrenia. Please visit to Dr.
Javitt's interview page to view his comments. Sarcosine and Glycine Suppliers Both Sarcosine and Glycine are commercially available as a food supplement or nutritional supplements through a large number of private vitamin and supplement companies.
More Sarcosine and Glycine Information:
References: Begany, T. 2004. Emerging Schizophrenia Treatments Aim to Enhance NMDA Receptor Function. Neuropsychiatry Reviews Vol 5, No 6. Coyle JT and G Tsai. 2004. The NMDA receptor glycine modulatory site: a therapeutic target for improving cognition and reducing negative symptoms in schizophrenia. Psychopharmacology 174:32-28. Harrison PJ and DR Weinberger, 2005. Schizophrenia genes, gene expression, and neuropathology: on the matter of their convergence. Molecular Psychiatry 10:40-68 D-serine efficacy as add-on pharmacotherapy to risperidone and olanzapine for treatment-refractory schizophrenia - Biol Psychiatry. 2005 Mar 15;57(6):577-85. The NMDA receptor complex: a long and winding road to therapeutics - IDrugs. 2005 Mar;8(3):229-35. Glycine and D-cycloserine attenuate vacuous chewing movements in a rat model of tardive dyskinesia. - Brain Res. 2004 Apr 9;1004(1-2):142-7. Javitt DC and JT Coyle. 2003. Decoding Schizophrenia. Scientific American. Dec 15, 2003. Maguire GA. 2002. Comprehensive understanding of schizophrenia and its treatment. Am J Health Syst Pharm 59:(17 Suppl 5):S4-11 Moghaddam B and ME Jackson. 2003. Glutamatergic Animal Models of Schizophrenia. Ann. N.Y. Acad. Sci. 1003: 131–137 Augmentation strategies in the treatment of schizophrenia - CNS Spectr. 2001 Nov;6(11):904-11 Glycine modulators in schizophrenia - Curr Opin Investig Drugs. 2002 Jul;3(7):1067-72. Amelioration of negative symptoms in schizophrenia by glycine - Am J Psychiatry. 1994 Aug;151(8):1234-6. Additional List of Papers relevant to glycine, NMDA receptors and schizohprenia: D'Souza et al., "Glycine Site Agonists of the NMDA Receptor: A Review,"
CNS Drug Reviews, vol. 1, No. 2, pp. 227-260, 1995.*
|
Advertisement
|